The National Academies has released a new report, Mechanisms for Organizational Behavior Change to Address the Needs of People Living with Alzheimer’s Disease and Related Dementias.
The report is available here, and more detail form the National Academies is below:
Patients diagnosed with Alzheimer’s disease and related dementias (ADRD) rely on family members, their community, and the health care system for progressively increasing support over the course of their disease. These people receive care through a frequently siloed health care system across hospitals, nursing homes, ambulatory care settings, and long-term care settings, as well as community- and home-based care. As the number of people living with a diagnosis of ADRD continues to grow, so does the need to provide better support for these people and their caregivers. The National Institute on Aging (NIA) Division of Behavioral and Social Research suggests that organizational behavior change will be needed for health care systems to integrate all of the services and supports required to provide high-quality care for people with ADRD.
NIA sponsored a workshop hosted by the National Academies of Sciences, Engineering, and Medicine to explore mechanisms to improve the quality of care for people living with ADRD and the potential of innovative payment models to incentivize health care systems to make the necessary systemic changes. The workshop convened a diverse array of experts in fields including nursing, geriatrics, health care economics, health care services research, quality measurement, social work, medical ethics, law, health care finance, and health care policy. This publication summarizes the presentation and discussion of the workshop.
In April 2023, the Massachusetts hosted a webinar entitled “Exploring Age and Dementia Friendly Design for Our Built Environment: How to Optimize Health and Wellness Through Physical Infrastructure Design”
The unique safety and care needs of geriatric patients are receiving increased attention in hospitals, due in part to new state requirements for identifying patients with dementia and optimizing their care.
As the population of Massachusetts ages, the unique safety and care needs of geriatric patients are receiving increased attention in hospitals, due in part to new state requirements for identifying patients with dementia and optimizing their care.
Sturdy Memorial Hospital, a community hospital in Attleboro, started more than five years ago to develop better systems for emergency care of geriatric patients, work they have more recently expanded into inpatient units.
Other Massachusetts hospitals, including Boston Medical Center, are also finding they are already in good alignment with new requirements that went into effect this month directing acute care hospitals to have an operational plan for patients with dementia.
The law, signed by Governor Charlie Baker in 2018, was originally scheduled to go into effect in October 2021, but key provisions were postponed a year in deference to the pressures put on hospitals by the coronavirus pandemic.
Sturdy Memorial and BMC talk about their approaches
Dr. Brian Patel, who is an emergency physician, Sr. Vice President of Medical Affairs, Chief Medical Officer and Chief Quality Officer at Sturdy Memorial, is one of a number of champions of improved care for geriatric patients in the hospital setting.
Dr. Patel served on a workgroup convened by the Massachusetts Health & Hospital Association in 2018 to develop guidance for complying with the new law, which prompted Sturdy to implement recommendations from the MHA workgroup’s 2018 report ahead of the law’s effective date. “We knew this work needed to be done. We used the plan as a framework to start advancing our geriatric care,” he says.
Key takeaways
The law
As of October 1, 2022, a new state law mandates Massachusetts hospitals to create and implement a master plan for identifying patients with dementia and optimizing their care.
The background
Signed in 2018, the law was originally scheduled to go into effect last year but was postponed in deference to the pressures put on hospitals by the coronavirus pandemic.
Key takeaways
The context
As hospitals have prepared to comply with the law, many have found they already have at least some elements of a master plan in place.
The resources
Massachusetts Health & Hospital Association and the Alzheimer’s Association offer guidance for complying with the state law. Many hospitals also use resources from programs such as Nurses Improving Care for Health System Elders and Age-Friendly Health Systems.
Dr. Patel reports that Sturdy participates in NICHE — Nurses Improving Care for Healthsystem Elders — a program designed to enhance nurses’ knowledge and evidence-based practices in caring for older adults and has been working closely with the American College of Emergency Physicians, which accredited Sturdy as a Bronze Level 3 geriatric ED in 2018 and, more recently as a Silver Level 3 in 2022.
“The work we’ve been doing with ACEP and on and the inpatient side with NICHE overlaps with the Massachusetts requirements around management of dementia and delirium,” says Dr. Patel. Sturdy also uses components of the Age-Friendly Health Systems initiative offered by the John A. Hartford Foundation and the Institute for Healthcare Improvement.
Boston Medical Center also has leveraged a variety of resources to build an operational plan for geriatric and dementia care. Lisa Caruso, M.D., geriatrician and Director of Quality and Patient Safety in the Department of Medicine at BMC, says the hospital joined the Age-Friendly Health System program in 2017. Dr. Caruso recalls that creating a geriatric order set, implementing a mobility program and using the Confusion Assessment Method were among their first improvement projects. All address the issue of delirium, which Dr. Caruso says, “is one of the worst things that can happen for somebody who has dementia in the hospital.”
Optimal dementia care extends across six functional domains
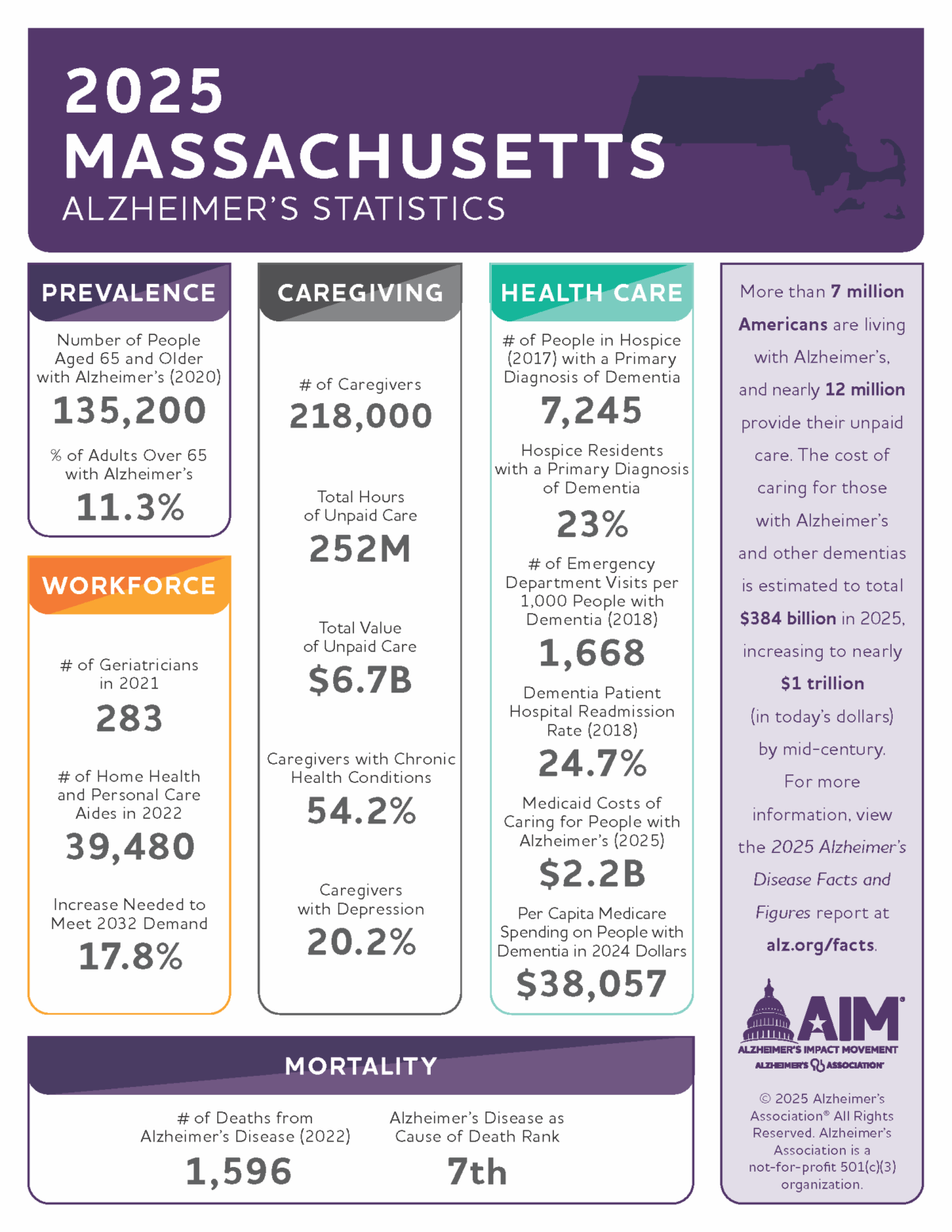
The Alzheimer’s Association estimates that the number of people ages 65 and older with Alzheimer’s dementia in Massachusetts will have increased more than 15% between 2020 and 2025 and that people with Alzheimer’s disease have almost twice as many emergency department visits and hospitalizations as seniors without dementia.
The MA Department of Public Health first issued recommendations for managing patients with dementia in acute care settings in 2017. Following up on its workgroup report from 2018, MHA published an operations “roadmap” in conjunction with the Alzheimer’s Association this summer.
The roadmap calls for attention to:
Advance care planning — including disease progression, health care proxy, advance directives and palliative care
Staff training — including all patient-facing staff, using resources from initiatives such as the Nurses Improving Care for Health System Elders
History, screening and assessment — engaging with the patient and care partner, assessing known and suspected diagnosis of cognitive vulnerability
Dementia-capable environment — prioritizing safety and minimizing use of chemical and physical restraints
Treatment and management — preventing delirium, managing dementia and delirium when it occurs
Transfer and discharge — optimizing intra-hospital transfers, to/from outside facilities and home
Liz McCarthy, Health Systems Director at the Alzheimer’s Association, New England region, explained during a webinar co-produced with MHA, that hospitals need to work on all six domains simultaneously. “You’re not starting with one of these,” said McCarthy. “They’re all going to be happening at roughly the same time.” She also emphasized the importance of engaging with the patient’s care partner throughout the hospital stay and the role of senior leadership to sponsor and direct this wide-ranging effort. McCarthy served with Dr. Patel on the MHA workgroup in 2018.
Describing BMC’s operational plan, Deborah Whalen, R.N.P., Associate Director Quality and Patient Safety in the Department of Medicine at BMC, emphasizes collaboration among the hospital’s departments. This is particularly evident in planning for transitioning patients with dementia to discharge. “Because we’re a safety net hospital,” says Whalen, “we have always focused on transitions in the various settings. We often work with our community partners as we help our patients move them through the settings and back into the community.”
Whalen also reflects on how the state law helped her and her colleagues at BMC see the work they already were doing in a new light and showcase it in the operational plan. “The law requires that we have a plan available for the Department of Public Health to review, right? We went farther than that,” says Whalen. “We created a plan that is alive. Now when DPH comes, they can walk through our organization and see it in action.”
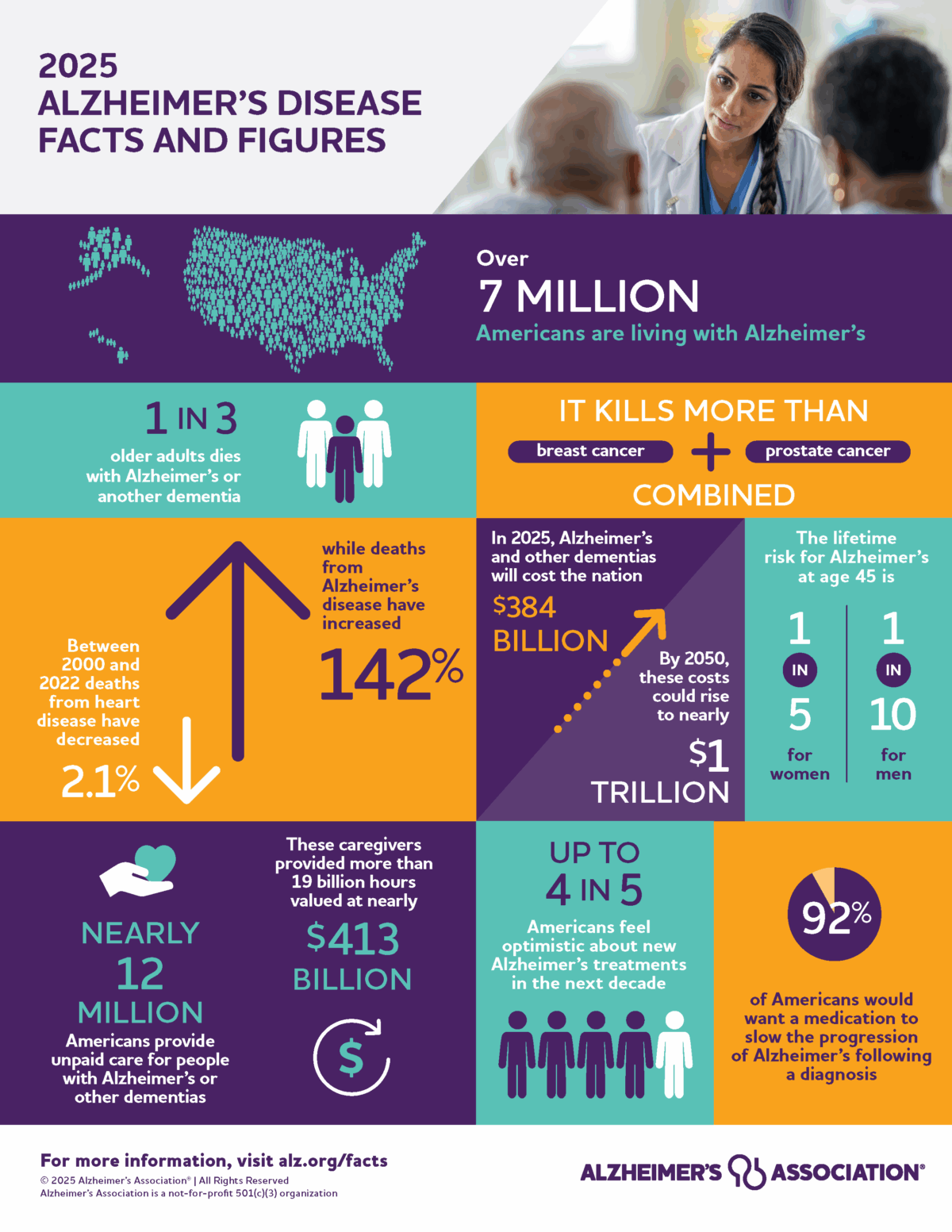
2025 Alzheimer’s Disease Facts and Figures is a statistical resource for U.S. data related to Alzheimer’s disease, the most common cause of dementia. Background and context for interpretation of the data are contained in the Overview. Additional sections address prevalence, mortality and morbidity, caregiving, the dementia care workforce, and the use and costs of health care and services.
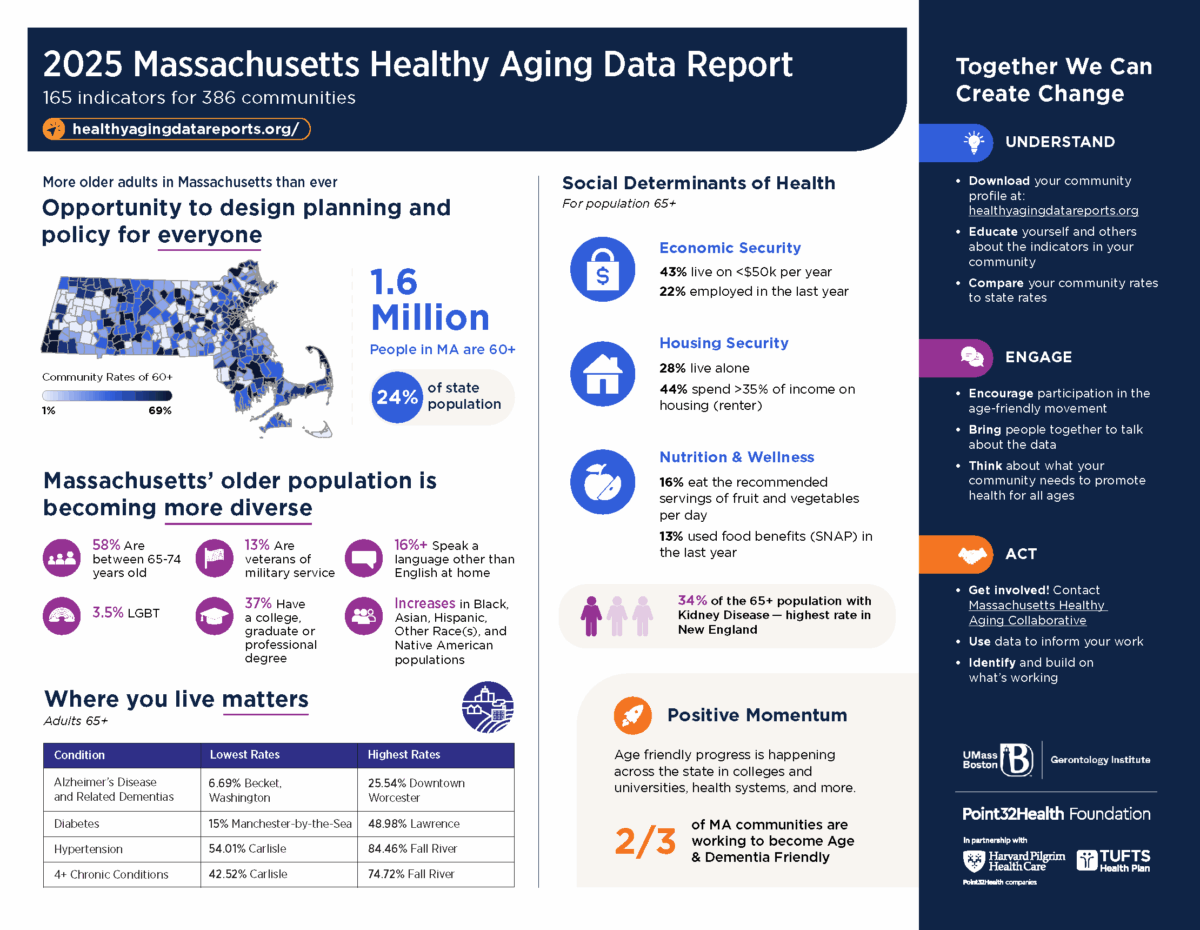
The 2025 Massachusetts Healthy Aging Data Report includes the following tools: • 386 community profiles (for every city and town and some urban neighborhoods) • 165 maps listing community rates for each indicator (organized alphabetically and ranked high to low) • 18 interactive web maps • Infographic summarizing key findings • Highlights Report • Technical documentation
This toolkit was developed by the Care Planning Team of the Massachusetts Advisory Council on Alzheimer’s Disease and All other Dementias (Council). Its goal is to facilitate the development of person-centered dementia care plans that support living well with dementia. Its target audience is the wide range of individuals involved in effective dementia care planning. These individuals include people living with dementia, dementia care partners, families, community-based service providers, and health care providers. It was developed to help readers understand:
the importance and benefits of person-centered dementia care planning;
the unique characteristics of dementia that necessitate person-centered care plans; and
what dementia care planning involves and includes.
In addition to guidance on dementia care planning, this toolkit provides examples of dementia care plans, and a section called “Dementia Care Planning Resources,” featuring links to helpful materials and tools, including those developed by the Council’s teams.
In September 2022, MHA and the Alzheimer’s Association introduced a roadmap to assist Massachusetts healthcare providers in preparing for the implementation of a state-mandated operational plan for Alzheimer’s and related dementias.
The state’s Alzheimer’s and Related Dementias Acute Care Advisory Committee – established by the legislature – in 2017 issued a report of recommendations to provide optimal care to persons with dementia in acute care settings. In 2018, these recommendations were incorporated into legislation and passed into law as Chapter 220 of the Acts of 2018: An Act Relative to Alzheimer’s and Related Dementias.
Section 8 of the law requires all licensed hospitals to complete and implement an “operational plan for the recognition and management of patients with dementia or delirium in acute-care settings.” In July 2021, the required date for implementation was extended from October 2021 to October 1, 2022, due to the COVID-19 pandemic.
The MHA roadmap outlines an operational plan for senior leadership, recommendations of who should be on the team to implement the plan; identification of the six broad categories of an operational plan and the pathways to take to implement it, and suggested outcome measures for ongoing quality assurance and performance improvement.
WATCH: MHA and the Alzheimer’s Association hosted a one-hour webinar, which includes case examples from hospitals implementing their own operational plans.
The National Academy of Medicine today launched Resource Compendium for Health Care Worker Well-Being, which highlights tools that are ready to be deployed and strategies to address systems issues related to health care workers’ burnout. The compendium, which is a product of the Action Collaborative on Clinician Well-Being and Resilience, of which AHA is a participant, organizes resources into six essential elements: advancing organizational commitment; strengthening leadership behaviors; conducting workplace assessments; examining policies and practices; enhancing workplace efficiency; and cultivating a culture of connection and support.
“Stress, trauma and burnout among front-line health care workers are at historic levels as we head into the third year of the pandemic,” said AONL CEO Robyn Begley, DNP, R.N., who serves on the collaborative’s steering committee alongside AHA President and CEO Rick Pollack. “Health care is, at its core, people caring for people. NAM’s detailed plans and actionable resources will help support well-being and resiliency of caregivers who continue to make sacrifices for all of us.”
The workgroup developing the compendium was led in part by AHA past-chair and Carilion Clinic President and CEO Nancy Howell Agee.
Registration is FREE for both ANA members and non-members.
You may soon be faced with one of the most challenging aspects of the COVID-19 pandemic: The need for nurses with little or no critical care experience being called on to be part of a team caring for severely ill COVID-19 patients, many of whom must be on a ventilator to survive.
A FREE, On-Demand Series for ALL Nurses – Part of the ANA COVID-19 Webinar Series
Taught by a highly experienced critical care nurse specialist and educator, this program focuses on key skills needed when caring for a COVID-19 patient on a ventilator. Content is presented in an easy-to-understand – and use — manner. After viewing this webinar, you will be better prepared to be an effective part of a team caring for critically ill patients on a ventilator.
This 60-minute on-demand webinar contains four sections that you can view all at once or one at a time. Topics include:
Basic ventilator settings and abbreviations such as rate, tidal volume, PEEP, and the modes of ventilation commonly encountered for patients with respiratory failure and ARDS
How to assess a patient on a ventilator: Important differences compared to routine patient assessments
Ventilator alarms: The how-to of ventilator alarm assessment and troubleshooting measures and interventions for apnea, high pressure (including how to suction a patient with an ETT), high minute ventilation, and low pressure/low minute ventilation